The dual burden of malnutrition, also called the double burden of malnutrition, occurs when a population suffers from both undernutrition and overnutrition (overweight and obesity) at the same time. In low-income countries, the focus is often undernutrition, but in fact overweight and obesity can now be found in most, if not all, countries, making malnutrition a more prevalent and complex issue for global health. (See a recent The Lancet survey here.) In the summer of 2019, two of our colleagues specializing in nutrition were preparing to write proposals for dual burden of malnutrition programs, particularly one expected in the Middle East. They needed evidence, and they needed it soon. We took the opportunity to pilot a newish approach to rapid evidence review (described in full here). In this post, we report some of the findings from the review. After presenting the methods (specific to this review) and results, we provide summaries of selected systematic reviews, and then discuss the findings before concluding with some limitations. It’s a long post, so please jump to the section that interests you!
The rapid evidence review approach we used focuses on systematic reviews and evidence maps. Systematic reviews and evidence maps collect and synthesize or catalogue information from relevant primary studies. In this rapid review we also looked at a subset of primary studies conducted in low- and middle-income Middle Eastern countries (not reported here). The review question we agreed with our colleagues is: What evidence do we have about programs and policies that address the dual burden of malnutrition for neonatal through youth plus maternal populations, especially double-duty interventions but also interventions that focus specifically on overweight and obesity, in low- and middle-income countries (LMICs)? The two of us conducted this review, starting from the initial meeting with our “clients” to submitting the written report and appendixes to them, in six weeks.
Methods
Search
With the help of our FHI 360 reference librarian, we searched the PubMed, Scopus, Web of Science and POPLINE indexes. We also used the EBSCO portal to search an additional seven indexes. Box 1 presents the search string we used for PubMed.
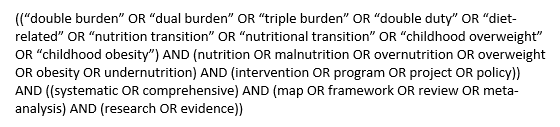
Box 1. Dual burden of malnutrition search string employed in PubMed
At the same time, one of us conducted a website search covering 16 websites, including those specializing in systematic reviews, evidence maps and international development impact evaluation evidence. The full list of indexes and websites along with the number of hits from each is available upon request. The reference librarian exported the search results to EndNote, and we imported these into Covidence for screening. We conducted title and abstract screening of the website hits while searching them and then uploaded the screened results into Covidence.
Screening
For title and abstract screening, we excluded studies where any one of the following criteria was clearly met. A single reviewer screened each study.
- Published before 2004
- Abstract not in English
- Does not include any studies from LMICs
- Not a review study
- Not completed (i.e., is a protocol or title)
- Does not concern policies, programs or interventions
- Does not include empirical studies
- Does not cover populations including prenatal through youth or pregnant and lactating women
- Only concerns undernutrition
- Does not include any outcomes related to nutrition or health
- Only includes pharmaceutical or surgical interventions
For full-text screening, we excluded studies according to the following criteria.
- Full text not available to us
- No included studies
- Title, protocol or brief
- Only methods
- Only portfolio
- Not in English
- No included studies from LMICs
- Only prevalence or burden
- Wrong populations (meaning age ranges)
- Does not include empirical studies
- No systematic search or pre-defined inclusion criteria
- Wrong outcomes
As we began to realize that a large number of systematic reviews would be eligible after full-text screening, we tagged eligible studies at this screening stage if they have less than 10% of their included studies conducted in LMICs or if they are etiology-only studies. A single reviewer screened each full text. Both reviewers discussed and came to agreement in all cases of uncertainty.
Coding
Because 210 systematic reviews and umbrella reviews passed the full-text screening stage, it was not possible to code all eligible studies in the limited period of time for the rapid review. We thus restricted the coding to reviews with 10% or more included studies conducted in LMICs and reviews including intervention studies (i.e., not exclusively etiology studies). We expected that these would be the most relevant for our colleagues’ program design purposes. We included all umbrella reviews that include intervention studies. After these restrictions, we coded 12 umbrella reviews and 66 systematic reviews.
Table 1 presents all the items coded. A single reviewer coded each study, and both reviewers discussed and came to agreement about any uncertainties.
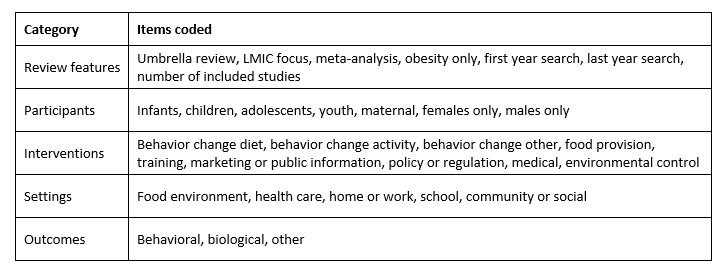
Table 1. Summary of items coded for 78 umbrella and systematic reviews of intervention studies
Obesity-only means that the review focuses only on overweight- or obesity-related outcomes. Among the intervention types, food provision includes supplements and changes in food composition. If a review only included surgical or pharmacological interventions, we excluded it, but if a review included interventions in those categories (“medical”) and interventions in our included categories, we included it. Thus, the medical category captures combination reviews. The World Health Organization and others have emphasized that the drivers, and thus the possible solutions, to double malnutrition can be specific to different settings (WHO, 2017). To capture this information, we coded the settings covered by each review.
Critical appraisal
We critically appraised the included reviews using the ROBIS tool (Whiting et al., 2015). We selected this tool because it allows for greater judgment on the part of the appraiser to determine the level of concern. Other tools use more restrictive questions better suited to reviews of medical studies. The possible ratings are low concern for bias, unclear concern for bias and high concern for bias. We tested the critical appraisal by having both reviewers appraise the same three studies. There was disagreement on the final rating for one of those three. After discussion, we both appraised a second set of three studies. There was agreement on the final ratings for all three. Then, a single reviewer appraised each study, and both reviewed, discussed and came to agreement about any uncertainties. We expected that we would not have time to critically appraise all 78 studies, so we ordered the studies with umbrella reviews first and then most recent to oldest, and appraised them in that order.
Results
Figure 1 displays the PRISMA flow diagram for our search and screening.
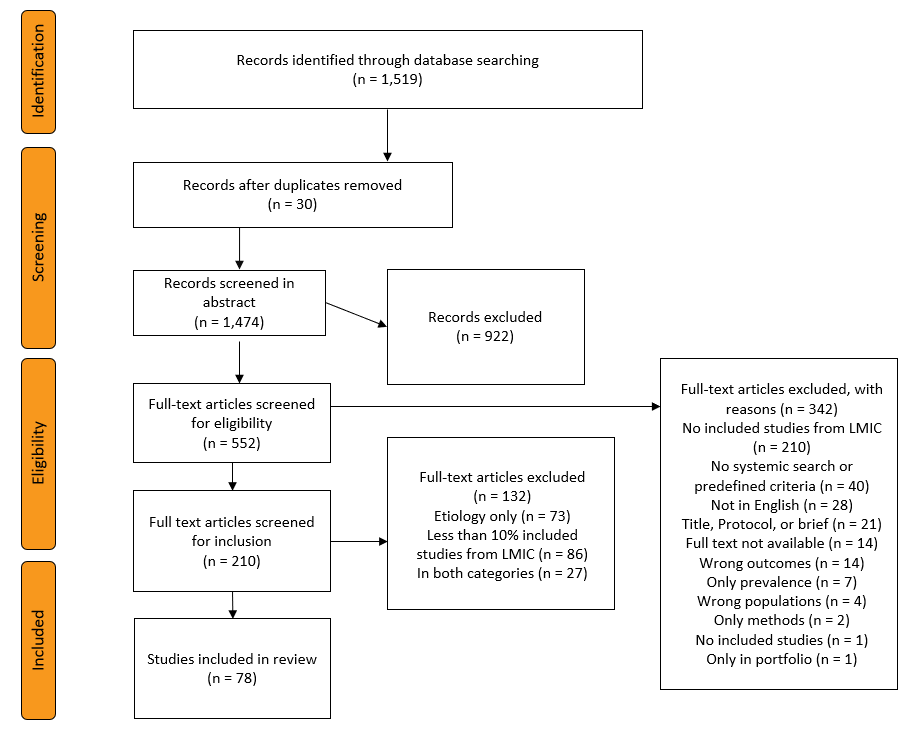
Figure 1. PRISMA flow diagram
We were able to assess 48 reviews for risk of bias. The most common concern from our appraisals is that, even when the reviewers appraise risk of bias for included studies, they don’t account for it when conducting synthesis. Other common concerns are vote counting in the synthesis and limited search strategies. Of those we appraised, 15 have high concern for bias, four unclear, 24 low, and five stated that the review has no conclusive results, so we did not appraise them to allow for more appraisals in the limited time.
We found 66 systematic reviews of relevant intervention studies. Figure 2 presents the evidence map for all the (non-umbrella) systematic reviews by intervention category and setting category. The map shows that there is a large number (55) of reviews that include diet-related interventions and a large number (55) that include activity-related interventions. Forty-seven reviews include both. This finding is likely a result of the large number of reviews focused on prevention and treatment of obesity. There are 48 reviews that cover school settings; 38 community or social settings; 29 home settings; 24 health care; and two food environment. Although we labeled the category “home or work” in our coding form, we did not notice any reviews covering work settings, which is not surprising given our participant inclusion criteria.
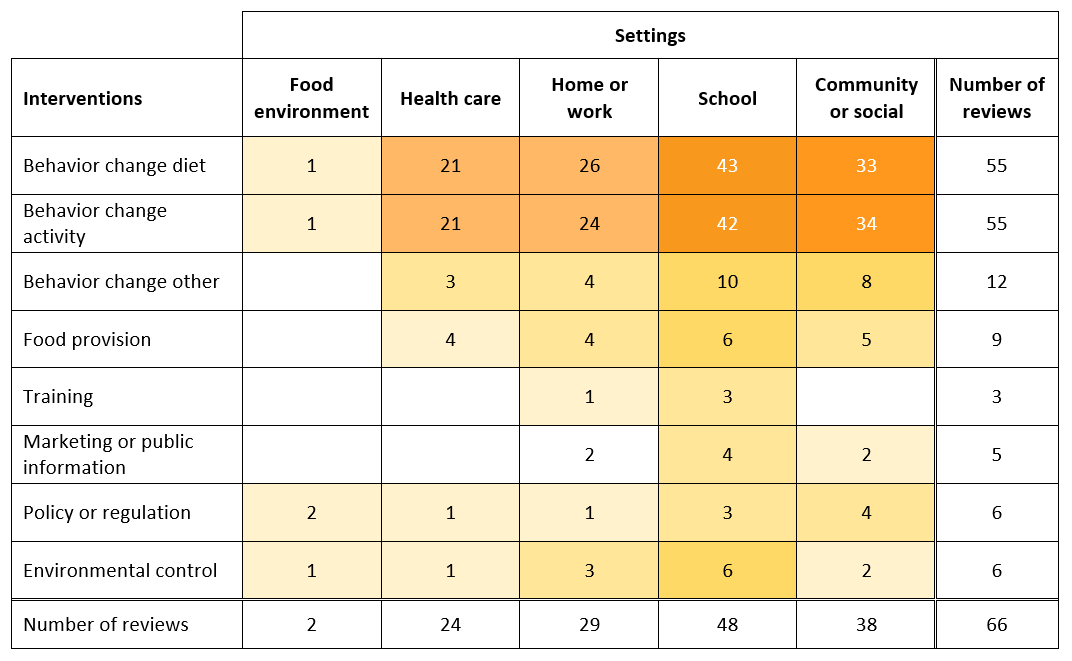
Figure 2. Evidence map: number of systematic reviews by intervention and setting
Although we did limit the included intervention reviews to those with 10% or more included studies from LMICs, most of these reviews still have a majority included studies from high-income countries. We did not extract data on which countries, but our impression is that most frequently seen LMICs in the reviews are Brazil, China, India, Iran, Mexico and Thailand (not in any order). We coded reviews as having an LMIC focus if they have a stated LMIC focus, are restricted to regions with many LMICs, or limited to specific LMICs. There are 13 such systematic reviews. In this subset, just as with the full set of reviews, we see that the interventions most reviewed are those designed to change diet and activity behavior, school is the more common setting and community or social is the next most common. We provide additional information about the LMIC-focus reviews in this post).
Our colleagues are very knowledgeable about the evidence for undernutrition interventions but not overnutrition interventions, so our inclusion criteria allowed for reviews that only look at overnutrition, hence the obesity-only code, as well as those that cover both. As mentioned above, we found a large number of obesity-only reviews. In fact, of the 66 systematic reviews, only five reviews look at both undernutrition and overnutrition. We provided our colleagues with written summaries about the findings of these five reviews, which we share below.
Summaries of included systematic reviews covering both undernutrition and overnutrition
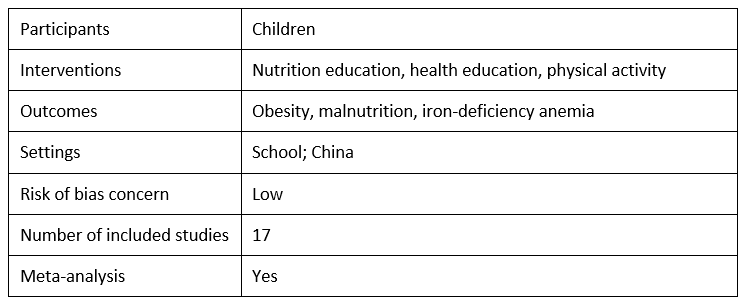
Limitations of studies on school-based nutrition education interventions for obesity in China: A systematic review and meta-analysis by Kaimeng Kong, Jie Liu and Yexuan Tao, 2016
In this systematic review, Kong et al. review the evidence for school-based nutrition education to prevent obesity, focusing on primary school students in China. They present a meta-analysis of 17 included studies to analyze the effectiveness of school-based nutrition interventions in preventing obesity, malnutrition and iron-deficiency anemia. The authors find that there is no significant impact of nutrition interventions on obesity, which they attribute to limitations in their included studies. When they exclude studies with dissimilar baseline characteristics and selection bias, there is a statistically significant effect of nutrition interventions on obesity. Furthermore, when they stratify by duration of the intervention, they find that the intervention is effective only when it lasts more than two years, suggesting that the impacts of nutrition interventions on obesity may only be apparent for long-term interventions. Kong et al. do find that interventions aimed at preventing malnutrition and iron-deficiency are effective.
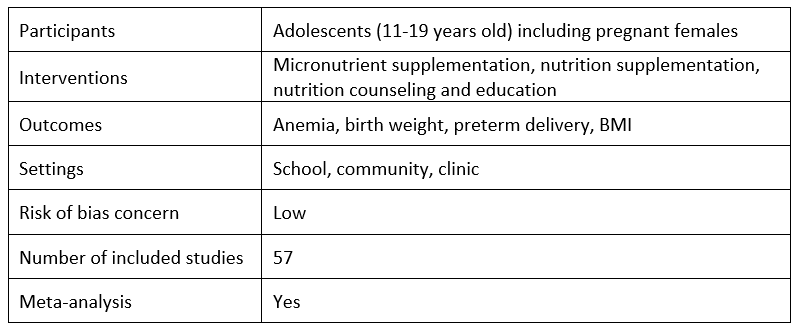
Interventions to improve adolescent nutrition: A systematic review and meta-analysis by Rehana A. Salam, Mehar Hooda, Jai K. Das, Ahmed Arshad, Zohra S. Lassi, Philippa Middleton and Sulfiqar Bhutta, 2016
Salam et al. review evidence for the effectiveness of nutrition promotion interventions among adolescents, including micronutrient supplementation, nutrition interventions for pregnant adolescents, and obesity prevention. They conduct meta-analyses for each type of intervention. They find that for adolescent (mostly females), micronutrient supplementation can significantly decrease anemia and for pregnant adolescents, nutrition interventions can significantly improve birth weight, and decrease low birth weight and preterm birth. Salam et al. also conclude that nutrition promotion interventions for obesity prevention have a marginal impact on body mass index (BMI), but that these findings are mostly from high-income countries which limits the generalizability to LMICs. This review is one of the few reviews that looks at micronutrient supplementation for adolescents.
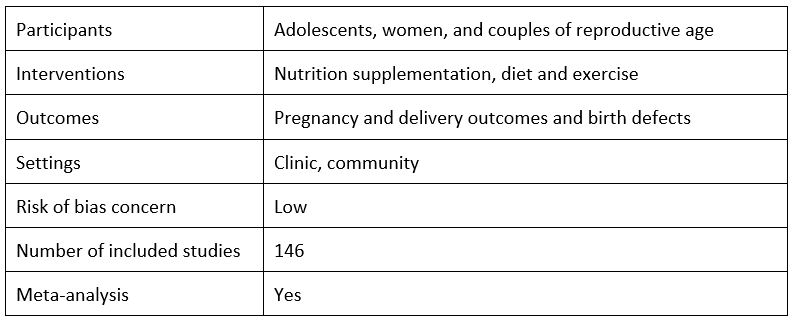
Pre-conception care: Nutrition risks and interventions by Sohni V. Dean, Sohra S. Lassi, Ayesha M. Imam and Zulfiqar A. Bhutta, 2014
In this systematic review and meta-analysis, Dean et al. begin by reviewing studies that examine nutritional risks, meaning the pregnancy outcomes correlated with pre-pregnancy weight, both underweight and overweight. They conclude that both maternal underweight and maternal overweight are associated with higher risk of unhealthy outcomes, including preterm birth and small-for-gestational age babies for underweight and preeclampsia and caesarean delivery for overweight. Dean et al. then review the effectiveness of interventions to target maternal weight during the pre-conception period. They find strong positive evidence for folic acid supplementation and emerging evidence for positive outcomes from micronutrient supplementation. The included trials of obesity interventions support interventions combining diet, exercise and support for pre-conception weight loss.
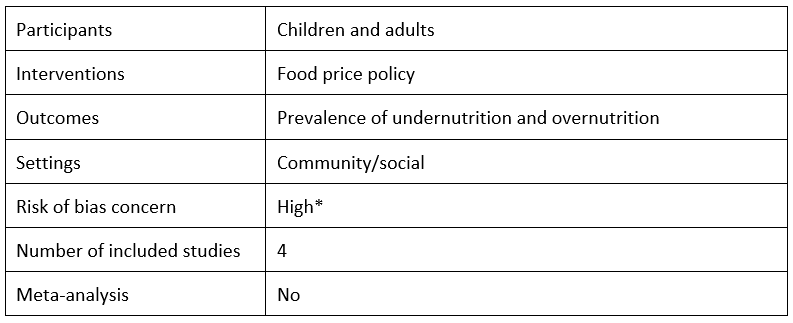
Can nutrition be promoted through agriculture-led food price policies? A systematic review by Alan D. Dangour, Sophie Hawkesworth, Bhavani Shankar, Louise Watson, C.S. Srinivasan, Emily H. Morgan, Lawrence Haddad and Jeff Waage, 2013
Dangour et al. review the evidence of the impact of national or international agricultural policies that affect the price of food on the prevalence of undernutrition- or nutrition-related chronic disease in children and adults. They include four studies, one each from Egypt, India, the Netherlands and United States; however, only the India study includes children. While the authors find some evidence that agriculture development and food production policies can affect the prevalence of undernutrition- and nutrition-related chronic diseases, they conclude that there is limited high-quality direct evidence on the impact of these policies on nutrition.
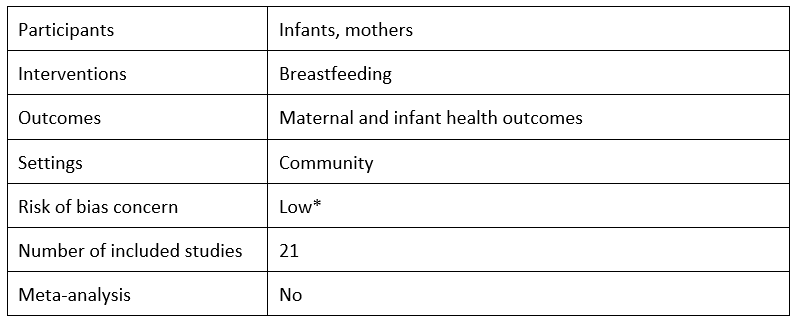
Optimal duration of exclusive breastfeeding by Michael S. Kramer and Ritsuko Kakuma, 2012
This Cochrane review by Kramer et al. reviews the impact of six month-exclusive breastfeeding versus three/four month-exclusive breastfeeding with mixed breastfeeding afterwards up to six months on child health, growth, and development, and on maternal health. The authors conclude that exclusive breastfeeding may have several advantages. Specifically, they find that exclusive breastfeeding for six months “reduces gastrointestinal infection and helps the mother lose weight and prevent pregnancy” (p. 1). However, Kramer et al. find no long-term impacts of exclusive breastfeeding on obesity, allergies, cognitive ability or behavior.
Discussion
Overall, the systematically reviewed evidence base for addressing the dual burden of malnutrition is small, particularly for LMICs. In our rapid review, which was conducted in the summer of 2019, we found only five systematic reviews that include 10% or more included studies from LMICs and cover both undernutrition and overnutrition interventions. Only one of these focuses on LMICs – the review summarized here on school-based nutrition interventions in China.
Considering all 66 included systematic reviews, there are many reviews for each of the settings; the exception is the food environment setting, for which there are only two reviews. Not surprising given our focus on children and youth, the largest number of systematic reviews covers interventions carried out in schools. The bigger gaps in evidence are across the types of interventions. The vast majority of the research reviewed studies diet and activity interventions, and there is also quite a lot about other types of behavior change. There is less reviewed evidence on food provision, training, marketing or public information, policy or regulation, and environmental control.
Limitations and conclusion
The limitations for this review include those associated with the shortcuts in the approach to make it rapid. Perhaps the most notable is that the screening and coding was only conducted by a single reviewer for each record. Because our topic was related to health, we found a large number of systematic reviews, which left us with little time to synthesize them and to review primary studies. We did map and catalogue the systematic reviews, and we extracted and mapped all the primary studies conducted in Middle Eastern countries (not reported here). Also, any review of reviews misses the most recent evidence, as the primary studies included in a systematic review will be at least a year older than the review publication date.
As noted in our companion post about this pilot review, our colleagues were not disappointed by the lack of synthesis, because they wanted to look at the systematic reviews themselves. But they did say they wanted us to be more prescriptive in terms of which articles they should read. We essentially gave them a big menu of articles with the features described, but they also wanted our recommendations.
Another limitation when considering the needs of our colleagues is that the intervention studies most included in systematic reviews focus on testing the intervention, or mechanism, and do not study delivery. Our colleagues needed information both about interventions and about delivery to guide their program design.
In the third post in this series, we summarize the findings from the included reviews that focus on LMICs.
*This systematic review was not critically appraised for the rapid review. We appraised it for the purpose of this blog post.
Photo caption: World Health Organization illustration of the dual burden of malnutrition
Photo credit: World Health Organization/CC BY-NC-SA 3.0 IGO license