The approaches used in the fight against HIV/AIDS have developed and changed over the past 30 years to reflect our increasing understanding of the nuanced interplay between biomedical and behavioral drivers of, and interventions for, the disease. As we enter what all hope to be the last decade of the epidemic, HIV/AIDS programming has expanded to also address structural factors that affect HIV acquisition and treatment. Household economic strengthening (HES) interventions include a range of economic interventions, focused on vulnerable households and individuals, that aim to address economic wellbeing and influence the economic determinants of HIV risk. Increasingly implemented as part of multi-sectoral programming, HES interventions have the potential to reduce sexual risk behaviors and improve care and treatment outcomes.
The linkages between economic strengthening and HIV outcomes
Both evidence and theory suggest that distal structural factors like economic vulnerability can contribute to proximal determinants of HIV risk and serve as barriers to treatment (Figure 1). To address these structural factors, governments, donors, and implementers have started including a range of standard economic development interventions, like cash transfers, savings groups, income generating activities, and vocational training, in HIV/AIDS programming. Many of these programs have been evaluated, but until recently the evidence on the effects of integrating HES into HIV programming had not been consolidated in a systematic way that could inform both programming and research efforts.
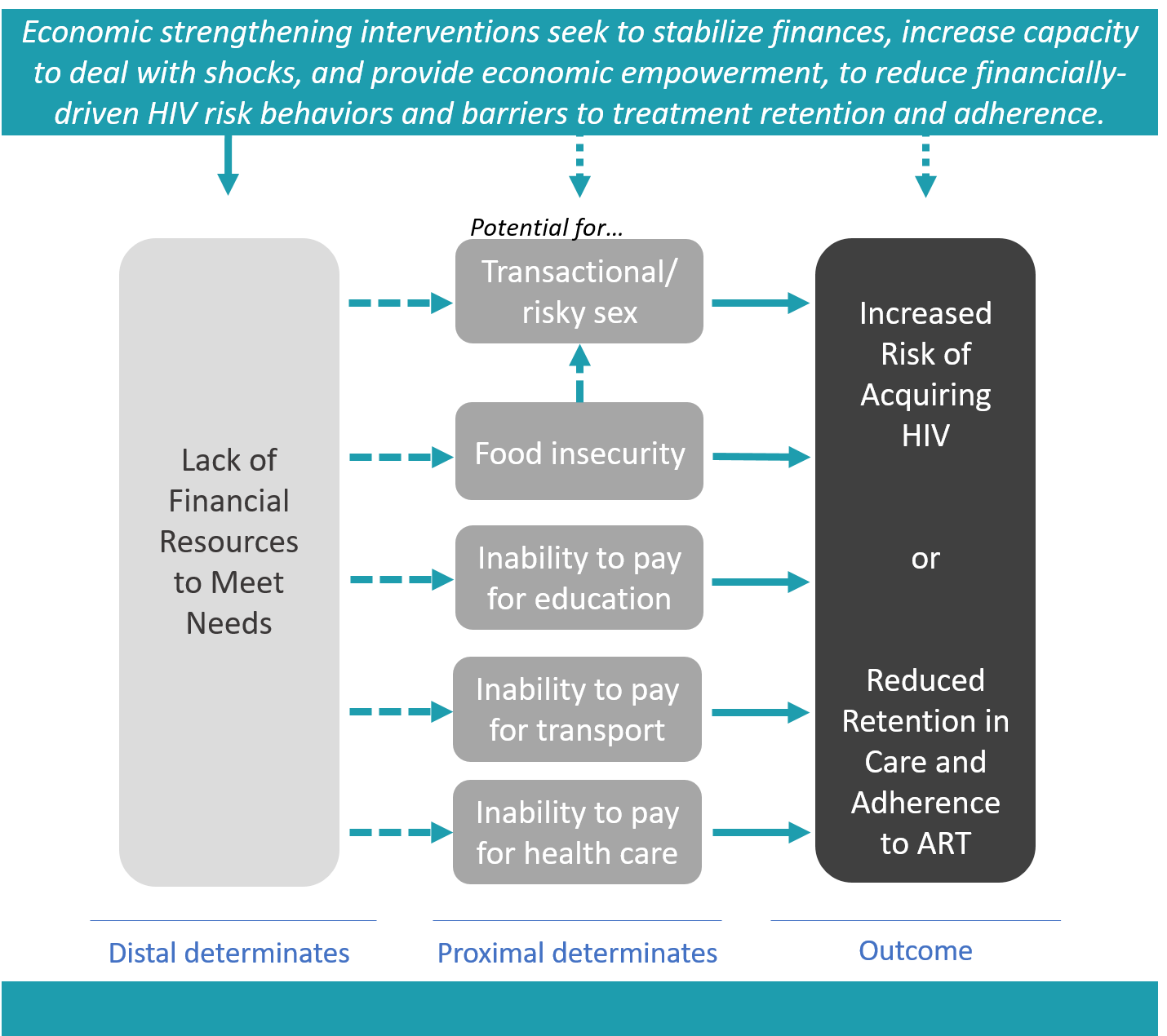
Figure 1: A few examples of pathways through which structural determinants affect HIV outcomes
ASPIRES addressed this gap by first conducting a systematic review of the evidence and then holding an expert consultation to reflect on the state of the evidence and define priorities for the field going forward.
The methods and the map
Swann presents the results of the systematic review in an evidence map using a matrix of 15 economic strengthening interventions crossed with 10 HIV outcomes. The map contains 108 articles and reports placed into cells coded for direction of effect, study quality, and whether the study assesses the effects of the HES intervention independently or in combination with other program elements.
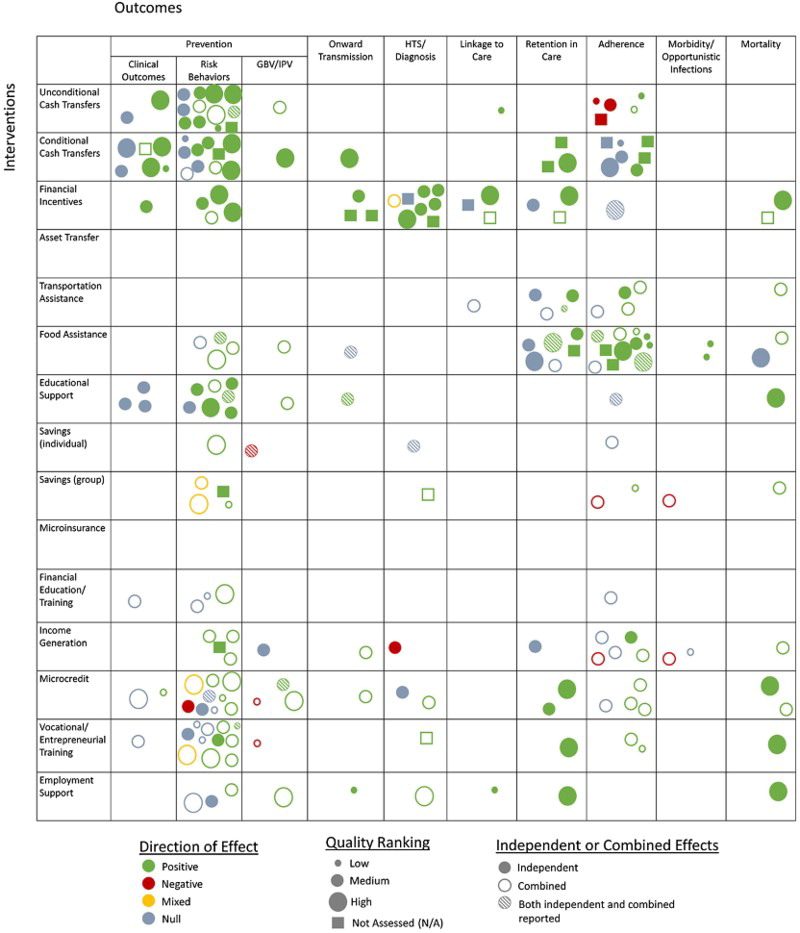
Figure 2: HES for HIV outcomes evidence map preview – source: Swann, 2018
Given the variation in important study characteristics, including differences in study design, outcome indicators, and analysis methods, Swann determined meta-analyses were not appropriate for this body of literature. Instead, her comparisons that inform the review results are descriptive in nature. Individual findings for quantitative analyses are classified as positive or negative only if the results are significant according to a p ≤ 0.05 threshold; null findings include those that did not meet this threshold. For qualitative studies, results are classified as positive or negative based on the qualitative data and interpretations presented.
Swann’s evidence map (Figure 2) is an impressive visual orientation to the breadth and depth of what we know about HES for HIV outcomes, and clarifies where there remain gaps in our knowledge. Her findings from the evidence review are presented in three articles according to clusters of outcomes that reflect 1) HIV prevention, 2) HIV testing and linkage to care, and 3) treatment adherence and retention; the methods and overarching results for her full review can be found in the first article.
What does the evidence say?
The first article, titled “Economic strengthening for HIV prevention and risk reduction: A review of the evidence,” assesses three HIV outcomes: clinical outcomes of HIV/STI incidence or prevalence, behavioral risk factors such as self-reported condom use or partner reduction, and known vulnerabilities such as gender-based violence or early marriage. This cluster of outcomes accounts for the greatest number of published results (n=64) and the strongest evidence base of the review. Swann assesses a wide range of HES intervention types in relation to prevention outcomes, and the findings are particularly positive for interventions like cash transfers and financial incentives, which provide economic resources directly to recipients. However, most of these studies rely on self-reported risk behavior change indicators. Beyond these “provision” interventions, where the causal link between intervention and outcome is relatively immediate and direct, Swann finds the evidence is less robust and sometimes mixed according to population group studied.
In the second article, titled “Economic strengthening for HIV testing and linkage to care: A review of the evidence,” Swann reviews results from 20 publications. She finds that financial incentives are consistently and independently linked with higher testing uptake and yield among adults and may also be beneficial for linkage to care following diagnosis. The discrete nature of financial incentives intuitively matches these more discrete services; perhaps unsurprisingly then, Swann notes evidence for other types of economic strengthening approaches related to testing and linkage to care is too sparse to identify any trends.
In the third article, titled “Economic strengthening for retention in HIV care and adherence to antiretroviral therapy: A review of the evidence,” Swann reports that most of the 38 publications reviewed measure an adherence outcome, while fewer measure retention in care, morbidity, and/or mortality. Here again, most of the studies focus on provision interventions, where the evidence generally trends positive. Evidence is more conclusive for self-reported and clinically-documented behaviors (such as medication pick up), compared to changes in CD4 counts and viral suppression.
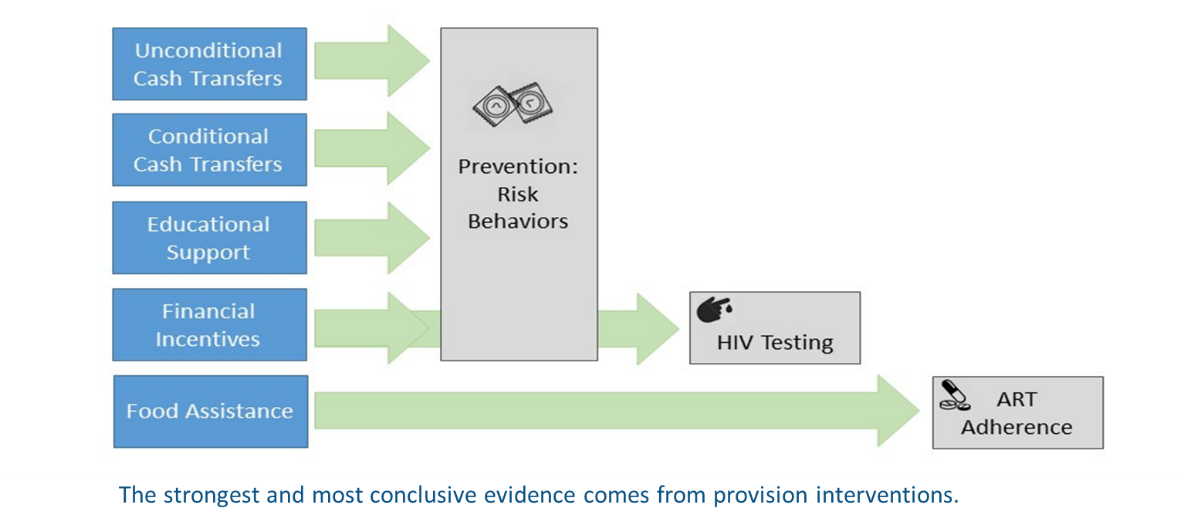
Figure 3: High-level findings of HES for HIV outcomes evidence review
Across Swann’s review there are also a number of caveats and limitations that help to further define and articulate what we do and don’t know about HES for HIV. For instance, she notes that our ability to compare and aggregate findings across studies – even those that fall within the same cell of the evidence map – is constrained by the differences in geography, target population, and intervention implementation, dosage, and scope among projects. There are also study design issues: few measure clinical outcomes, fewer have statistical power to do so, and many are reliant on self-reported behavioral data. And articles often lack a clear description of the (theorized or actual) pathways by which interventions are/not affecting HIV outcomes, leaving us to wonder what may have happened to create a particular result.
Where do we go from here?
Ultimately, as researchers, advocates, and policy-makers discuss important programmatic and scientific advances at AIDS 2018 and beyond, Swann’s evidence review offers an important reference to help align priorities around activities with maximum impact to help end the HIV epidemic.
Stay tuned for a future post that summarizes the supplement’s three original research articles that correspond to the three broader outcome areas of the evidence review!


