The Linkages across the Continuum of HIV Services for Key Populations Affected by HIV (LINKAGES) project developed an enhanced peer outreach approach (EPOA) to expand the delivery of HIV prevention, testing and treatment services to key populations including female sex workers, men who have sex with men, and transgender people who have not previously engaged in HIV programs. Since early 2017, more than 21 countries have implemented EPOA to reach key population individuals who have not engaged in an HIV program and link them to testing and treatment, if positive. Early EPOA findings from Burundi, Cote d’Ivoire and the Democratic Republic of Congo recently published in PLOS ONE show a higher statistically significant level of HIV case finding with those who were tested through EPOA compared to standard testing. Given that all HIV programs are striving to reach the UNAIDS 90-90-90 goals – 90% of people living with HIV know their status, 90% of those infected with HIV are on treatment, and 90% of those on treatment are virally suppressed – it is important to share our results with others.
What is EPOA?
EPOA is based on the concept that expanding and incorporating peers who are not formally part of the community-based HIV program may reach unidentified, harder-to-reach, high-risk key populations, resulting in higher rates of seropositivity (i.e., finding more people that are HIV positive). EPOA incorporates performance-based incentives and works through social networks to improve HIV case finding. EPOA is an additional component to an already established peer outreach program that provides a standardized prevention package (e.g., condoms/lubricants, screening for sexually transmitted infections, psychosocial and risk-reduction counselling) for key populations. The referral chain is detailed in Figure 1 below.
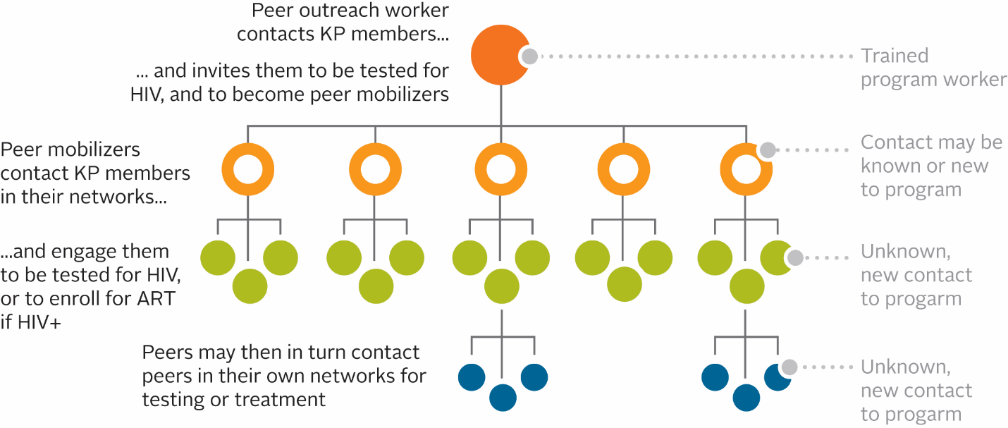
Figure 1: EPOA referral chain
Evaluation methodology
Our team piloted EPOA among female sex workers in Burundi, and among both female sex workers and men who have sex with men in Cote d’Ivoire and the Democratic Republic of Congo (DRC). EPOA implementation ranged from five to nine weeks – nested within a three-month reporting period. We suspended standard outreach for the duration of EPOA implementation but resumed it thereafter.
We used summary service statistics to compare HIV seropositivity (i.e., the number of new positives) from the EPOA implementation quarter to the two prior quarters which used only standard outreach. Then, we analyzed trends between the EPOA and standard outreach quarters and tested differences in proportions of HIV seropositivity using Pearson’s chi-square test. We considered p-values of less than 0.05 statistically significant.
Key findings
Our findings also show consistency in HIV seropositivity trends during standard outreach among both female sex workers and men who have sex with men across all three successive quarters. However, seropositivity increased when we introduced EPOA, which meant EPOA identified new HIV-positive cases. This finding is illustrated in the figure below from our paper.
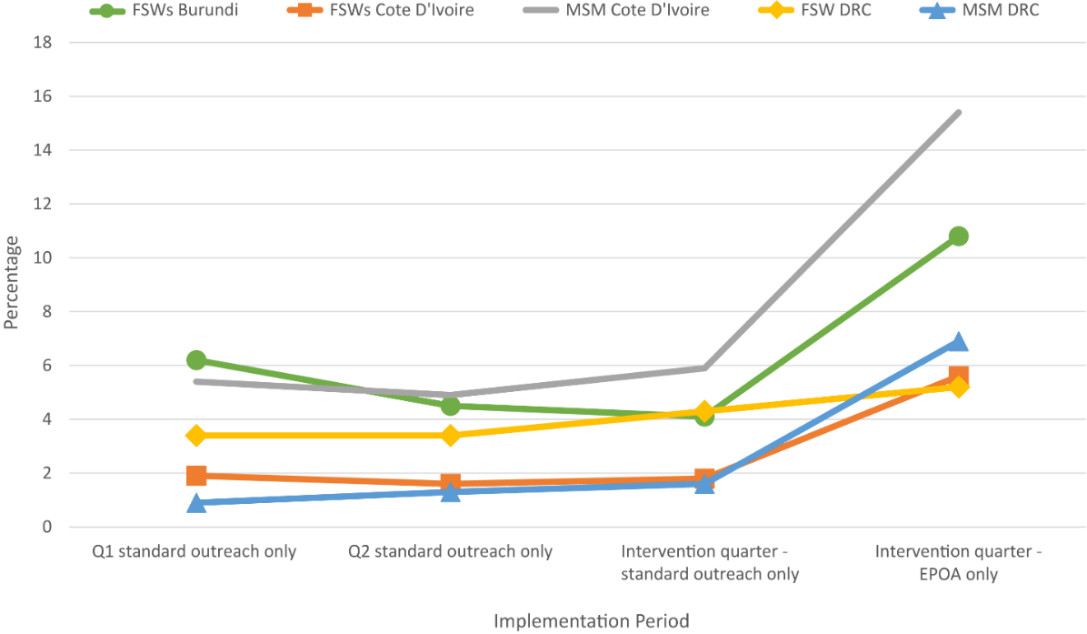
Figure 2: Trends in HIV seropositivity with standard outreach compared with the EPOA for female sex workers (FSWs) and men who have sex with men (MSM) in Burundi, Cote d’Ivoire, and DRC, 2017 (Source: PLOS ONE)
Discussion
For me, the most exciting aspect of the EPOA project is that it met its aim in identifying more HIV cases compared to standard testing. Our team hypothesized that the existing HIV program’s peer educators repeatedly reached the same individuals, which then translated into lower risk for HIV transmission and lower HIV case finding. While this is our goal in HIV prevention, we also have a dual objective as HIV implementers to identify those who are HIV infected and initiate them into treatment.
EPOA strived to break out of the same social and sexual networks to reach other individuals within high-risk groups and encourage them to get tested for HIV. We then linked those individuals to needed HIV services and, if newly diagnosed HIV positive, initiated into life-saving treatment. We used incentives at key points of HIV implementation, such as newly registered into the program or HIV testing, as motivation for both peer educators and mobilizers to have them encourage their peers to seek services.
I offer a couple of closing thoughts. First, our evaluation provides evidence that EPOA is a public health approach with great potential for reaching new populations and ensuring that they are aware of their HIV status. Second, we, the authors, are all full-time implementers so translating our strong and exciting findings into a PLOS ONE peer-reviewed article was challenging given journals are more geared to publishing research than program results. However, we persevered and with the help of FHI 360 and USAID experts, we wrote a manuscript and succeeded in publishing it in a journal!
LINKAGES is a global project funded by the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) and the U.S. Agency for International Development (USAID).
Photo credit: GDJ/pixabay


