
This post is cross-published on the CTI Exchange blog.
We all remember the early days of COVID-19 – the rapid changes to our daily lives and routines; school and work closures; new restrictions and rules. The future of many aspects of our lives and work became uncertain. In our work at FHI 360 on contraceptive research and development, this included uncertainty about the future of new and ongoing clinical trials.
At the time we were asking ourselves: Should all clinical trials proceed? What are the ethical implications of continuing clinical trials? What are the implications of halting them? Should contraceptive clinical trials be a priority compared to other trials? These were some of the questions we grappled with when COVID-19 first hit, and our teams were scrambling to brainstorm contingency plans without a lot of initial guidance. It was a challenging time.
 When guidance was eventually provided by the U.S. Food and Drug Administration (FDA), it was broad and designed to mitigate the impacts of COVID-19. For example, protocol changes made to limit exposure to COVID-19 could be implemented immediately without Institutional Review Board (IRB) approval. In addition, any activity that could be done remotely was moved online: remote safety assessments, remote monitoring, remote training and remote auditing. Finally, FDA guidance emphasized the need to capture missing data due to COVID-19; for example, missed visits due to site closures or COVID-19 infection need to be tracked. In order to put these general, high-level guidelines into action, the clinical operations team at FHI 360 and our partners responded rapidly and thought creatively to adjust our approach.
When guidance was eventually provided by the U.S. Food and Drug Administration (FDA), it was broad and designed to mitigate the impacts of COVID-19. For example, protocol changes made to limit exposure to COVID-19 could be implemented immediately without Institutional Review Board (IRB) approval. In addition, any activity that could be done remotely was moved online: remote safety assessments, remote monitoring, remote training and remote auditing. Finally, FDA guidance emphasized the need to capture missing data due to COVID-19; for example, missed visits due to site closures or COVID-19 infection need to be tracked. In order to put these general, high-level guidelines into action, the clinical operations team at FHI 360 and our partners responded rapidly and thought creatively to adjust our approach.
Site-level impacts and adjustments
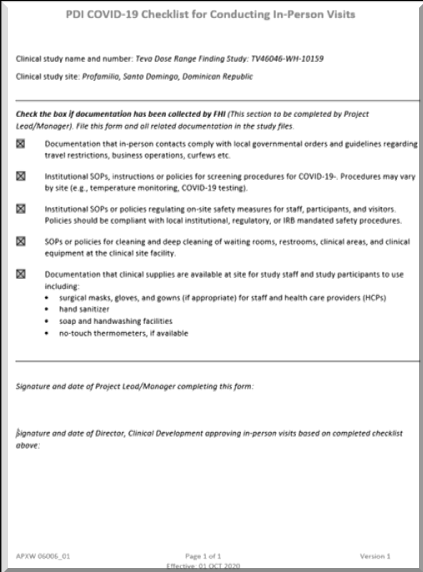 For some studies, in-person clinic visits were conducted over the phone instead of in person. Depending on the needs of the site, case report forms (CRFs) were modified to be phone-based and/or for electronic data capture. Physical medical exams were not possible, so researchers relied on self-reporting and self-testing; for example, participants were asked to locate their IUD strings and report back and were provided with home-based pregnancy tests via mail. Once sites opened up again for in-person visits, we developed new work instructions, safety protocols, and questionnaires to screen for possible COVID-19 infection. At some sites, personal protective equipment (PPE) and COVID-19 tests were acquired, and, in some cases, informed consent forms were updated to warn about the potential risk of traveling to clinic sites. Training with site staff became virtual, which made it difficult to connect and get to know the team but was cost-saving and allowed for more participants to join in. Onsite monitoring and auditing also became remote, and the team had to determine the best way to monitor virtually while also maintaining full participant confidentiality. Luckily remote monitoring was already gaining popularity before COVID-19 hit. There are a number of secure cloud-based options available, including Veeva SiteVault, which is one our team found particularly useful. Overall, as we learned more about COVID-19, as local and institution-based policies were updated, and as infection rates fluctuated, these procedures and protocols changed regularly, making it essential for our team to think on our feet and remain flexible.
For some studies, in-person clinic visits were conducted over the phone instead of in person. Depending on the needs of the site, case report forms (CRFs) were modified to be phone-based and/or for electronic data capture. Physical medical exams were not possible, so researchers relied on self-reporting and self-testing; for example, participants were asked to locate their IUD strings and report back and were provided with home-based pregnancy tests via mail. Once sites opened up again for in-person visits, we developed new work instructions, safety protocols, and questionnaires to screen for possible COVID-19 infection. At some sites, personal protective equipment (PPE) and COVID-19 tests were acquired, and, in some cases, informed consent forms were updated to warn about the potential risk of traveling to clinic sites. Training with site staff became virtual, which made it difficult to connect and get to know the team but was cost-saving and allowed for more participants to join in. Onsite monitoring and auditing also became remote, and the team had to determine the best way to monitor virtually while also maintaining full participant confidentiality. Luckily remote monitoring was already gaining popularity before COVID-19 hit. There are a number of secure cloud-based options available, including Veeva SiteVault, which is one our team found particularly useful. Overall, as we learned more about COVID-19, as local and institution-based policies were updated, and as infection rates fluctuated, these procedures and protocols changed regularly, making it essential for our team to think on our feet and remain flexible.
Higher-level impacts and adjustments
At the level of sponsors and contract research organizations (CROs), many of the impacts were budgetary. The budget implications for clinical trials during COVID-19 were significant but not as impactful as originally expected. While additional funds were needed for PPE, COVID-19 tests and increased staff hours to manage remote monitoring, there were significant cost savings with reduced travel for staff. Sponsors and CROs also had to manage insurance and legal liability issues, which often involved proving that those overseeing the clinical trials were considering and putting in measures to ensure the safety of research study participants. This sometimes cost extra money and time.
The way forward
As we look back at the response of our team throughout these challenging times, there were certainly frustrations, but it was also a time for growth and rapid learning. Some of the remote aspects of clinical trials operations are quite effective and can increase inclusivity and decrease costs. Many of these, especially remote monitoring systems, will remain in place for the long-term. Finally, in meeting this challenge, we learned a lot about our clinical operations team. Their skills, dedication and experience showed and were much appreciated.
Photo credit: Luis Alvarez/Getty Images


