
Viral suppression of people living with HIV (PLHIV) is essential to healthy living and preventing transmission of the virus, and is most effectively monitored through a relatively new approach of viral load testing. USAID-funded HIV programs are required to have 90% of all PLHIV on antiretroviral therapy virally suppressed by the year 2020 (UNAIDS, 2014). To reach this goal, countries like Kenya must overcome several challenges to viral load testing scale-up, including obstacles transporting samples and commodity distribution (Lecher, et al., 2015), which is often much harder in remote areas of the country.
Our study will generate a model to replicate existing transportation systems in a geographic information system (GIS), then develop multiple new configurations of the transport system augmented with UAVs and compare the model outcomes. These results will help explain how different configurations of UAV and ground-based transportation are able to reduce the time taken between when the sample is drawn and when it reaches the laboratory. Generated with program data from 22 health facilities, these results can help stakeholders understand how to best prepare for utilizing UAVs in Turkana, and the methodology can help support other program implementers in understanding UAV potential.
Viral suppression and HIV service delivery in Turkana County, Kenya
Viral suppression is relatively new to HIV management globally, including Kenya, which started scale-up in 2014. According to the most recent Kenya Ministry of Health guidelines (MOH, 2016), all PLHIV should begin antiretroviral therapy within two weeks of diagnosis, and viral load tests should be conducted at months 6 and 12 after initiation, then once annually. If a patient is not virally suppressed, viral load tests will be done once every three months until viral suppression is achieved. By 2015, nearly 800,000 PLHIV in Kenya were on antiretroviral therapy, and 38% of them had at least one viral load test; 83% of those were virally suppressed (Lecher, et al., 2015).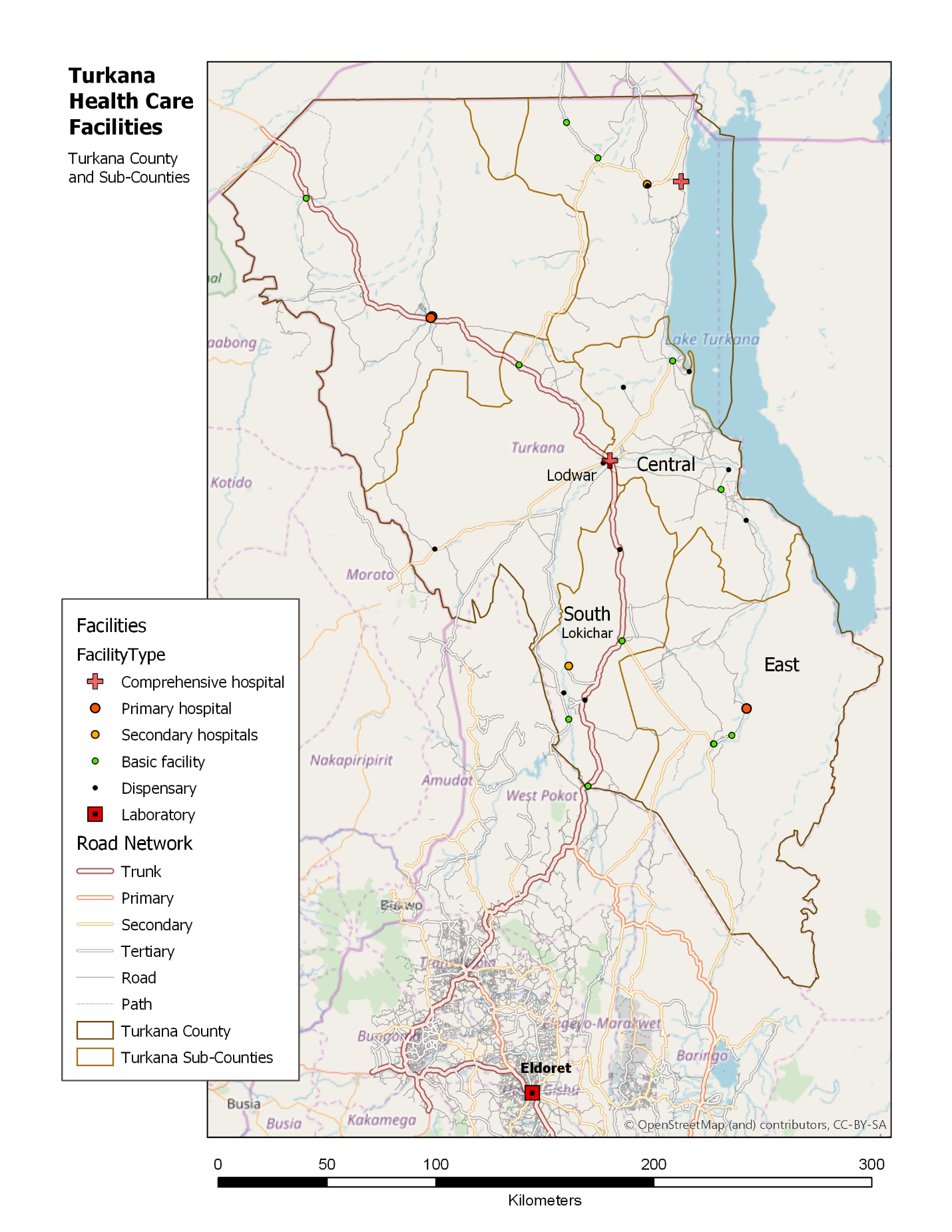
HIV Service Delivery and Support Activity (HSDSA), a five-year, USAID-funded, program operated by FHI 360 in Turkana and other counties, is responsible for HIV service delivery with specific tasks to increase the number of antiretroviral therapy patients that are virally suppressed through regular viral load testing, and to improve the capacity of commodity management and laboratory network services for testing. HSDSA supports 22 facilities providing HIV care and treatment in three of the six sub-counties: East, Central, and South (see map insert). Health workers collect samples using dried blood spots, a method lasting much longer and are more easily transported than whole blood without compromising quality. The HSDSA turn-around time goal for results is 10 days (described as the time between when the sample is taken to when results are provided to the patient).
Challenges to HIV viral suppression from transportation barriers
Health care workers at each facility are responsible for transporting samples themselves to Lodwar District Referral Hospital, where they are then taken via a secured courier service to the AMPATH laboratory in Eldoret, about 350 kilometers away. But the challenges faced by the current transportation system hinder HSDSA to meet their objectives, including viral suppression, in the following ways: (1) the turn-around times for viral load results are longer than the 10-day goal; (2) costs for transportation of samples are high; and (3) health facilities experience stock-outs of commodities related to viral suppression.
These barriers have a two-fold impact on viral suppression. Commodities that support suppression, including antiretroviral drugs (ARVs) and viral load test kits are delayed, causing stock-outs and preventing ARV adherence. And when samples – and subsequently test results – are delayed, the patient is unable to have timely, clinically-informed therapies to reach and maintain viral suppression.
Improving the transportation network in Turkana is essential to ensure antiretroviral therapy patients are virally suppressed, and doing so will require a combined use of proven approaches with new solutions. UAVs are one such tool that could be used in conjunction with current transportation networks to offer routine transportation for samples for remote health facilities in Turkana, but more evidence is required to understand the role UAVs may have.
UAVs as a solution for improving the viral load sample transportation system
With the obstacles faced by the current transportation system, the solutions are limited. Improving the road infrastructure, constructing bridges, and adding police patrols to these areas would certainly improve the ability to move quickly and freely between facilities, but these are not short-term solutions, and certainly not solutions that an HIV service delivery project could implement.
One potential solution to decrease these transportation delays that needs to be evaluated is the use of UAVs that could augment the current ground-based system. UAVs could provide the needed support when coupled with other cost- and time-saving approaches like using dried blood spots, gathering samples at intermediate or hub locations from multiple smaller facilities, and using functioning ground-based transportation for certain segments. This technology has progressed rapidly in recent years, and its ability to transport small payloads while avoiding rough and often impassible terrain holds great potential to address logistic challenges.
The existing evidence
As this technology is still nascent, only a few research studies have explored the potential cost, time saving, or impact of using UAVs to complement current laboratory and commodity transportation.
Phillips, et al. (2016) from VillageReach conducted a costing analysis that compared UAV-based transportation systems to ground-based transportation systems of laboratory samples from facilities to laboratories in Malawi. They modeled four scenarios to courier early infant diagnosis and/or viral load samples from facilities to the laboratory using UAVs or combining UAVs with current motorbikes to compare travel times and costs. They found higher costs and lower travel times when using UAVs, but note that UAV technology is ever improving, and costs continue to change with UAVs that have greater range and better fuel-efficiencies. Of note, the UAVs used for this modeling activity were battery-powered quad-copters with a range of 25 kilometers on one charge and a small payload of 500 grams; this UAV would not be feasible in Turkana as the distances between some facilities are more than 50 kilometers.
Haidari, et al. (2016) modeled the feasibility and costs for using UAVs to transport vaccines in Mozambique, finding that for distances under 75 kilometers, UAVs increased availability of vaccines and decreased logistic costs. Wright, et al. (2018) conducted a modeling exercise using the proportion of health facilities in a given area and estimated the volume of supplies needed, and used that information to generate basic costs for implementing UAV-based delivery. Others have conducted studies using small UAVs across short distances to determine how to use this technology to improve laboratory specimen transport, including Berman (2017) in South Africa, and Meier (2014) in Papua New Guinea, and Rabta (2018) studied UAV use for general humanitarian assistance in disaster scenarios.
While these studies are informative, they are not easily transferrable to the Turkana context because the distances between facilities that are most difficult to reach with ground-based transportation would be beyond the travel capacity of those UAV models, would not have enough capacity to carry adequate quantities of needed commodities, and may not support reverse logistics (i.e., pick up samples). Newer UAV models are currently being developed and tested that can transport larger quantities over greater distances, which could fit better in this area.
Our research design
The primary objective of our study is to understand how adding UAVs to the current transportation network for viral load samples (a) impacts turn-around time, and (b) at what transportation cost, through modeling a variety of transportation configurations. For the secondary objective, we seek to understand how the UAV-augmented transportation configurations for sample transportation (a) can improve the availability of HIV-related commodities at facilities to prevent stock-outs and (b) at what cost per unit for transportation.
Methods
By overlaying health facility-level demand data onto the current viral load sample transportation system, we will create an interoperable model that can be used to study UAV supported transport networks to reduce turn-around time.

Figure 1: Types of data used to develop the basis of the spatial model
The primary data set will contain facility-level characteristics, including volume of actual and expected tests per facility, number of antiretroviral therapy patients, volume of actual and needed HIV-related commodities, the costs for transportation of samples to reach the laboratory, and locations in latitude and longitude. Several types of data will be used to develop the basis of the spatial model, as shown in Figure 1, that will help us replicate ground-based transportation currently available, and plan UAV flight paths.
Additional locations will be added to the map including the laboratory in Eldoret, locations of warehouses where HIV commodities are stored, locations of airports where UAVs could be housed, and restricted airspace. Road network data sets, a digital elevation model, and land use/land cover data will be obtained from open sources. Information about the UAV models and specifications to use, and cost of operating UAVs for transport will be provided by our logistics company partner in Nairobi, Astral Aerial.
We will use program data from the past six months to generate a generic configuration of the transportation network, which will be used to describe current logistics, and will be the basis for comparing other UAV-augmented configurations. In the configuration representing the current transport network, each facility will have an average travel time to reach the laboratory along the road network, average cost for transportation of samples, average proportion of HIV-related commodities in stock, and average frequency by which samples and commodities are transported. By using actual data, the values represented in this configuration will inherently reflect the common delays faced in transportation.
We will then augment the configuration of the current transportation system with UAVs through multiple iterations. The configurations will be as realistic as possible, being guided by conversations with HSDSA and Astral Aerial. The different types of configurations will be based on two approaches:
- The UAV travels to intermediate locations to deliver supplies and pick up samples, and nearby facilities would use current ground-based transportation to pick up their supplies and drop off samples.
- The UAV travels to each health facility to deliver supplies and pick up samples.
To model each new configuration, we will consider the following: which facilities should serve as intermediate facilities, how many intermediate facilities should there be, in what order should facilities be visited based on volume and distance, where should the UAV be based, how frequently should the UAV travel to a given facility, should the UAV be used to take commodities from the warehouse or from an intermediate facility in Turkana, and should the UAV be used to take the samples to Eldoret or to an intermediate facility.
Once each configuration model is run in the GIS, we will have measures by health facility for viral load samples (the total travel time, frequency of trips, and volume per trip) and for commodities (the frequency of trips, volume per trip, and proportion of needed stocks). We will then determine the costs for the transportation of each sample and unit of commodity. This will provide information for designing the next configuration, and will allow us to consider how the frequency of transportation affects the volume and cost per sample. Thus, choosing the parameters for each configuration is a highly iterative process.
Analysis
The results of this work will inform FHI 360 staff, Ministry of Health, and other decision makers about whether transport of HIV-related laboratory samples and supplies in HSDSA-supported Turkana facilities could be impactful and cost-effective. Furthermore, we will present the model approach to the UAV community, and hope to support further programs in understanding the potential benefits of UAVs.
Photo caption: Women and children queue at a health clinic in Kapua, Turkana County, northwest Kenya
Photo credit: Russell Watkins/DFID / CC BY 2.0 license


